
- A PRESCRIPTION FOR HOPE PART 2 -
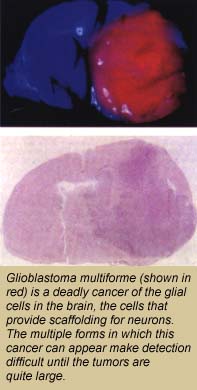 Glioblastoma multiforme is a cancer of the glial cells,
the cells that provide physical and chemical support for neurons.
Approximately 90-percent of all the cells in the central nervous system
are glial cells which, unlike neurons, undergo a cycle of birth,
differentiation, and mitosis (cell-division). That they undergo this
cycle, makes glial cells vulnerable to becoming cancerous. When they
do, as the name "multiforme" suggests, they can take on a wide variety
of different shapes, which often makes detection difficult until the
tumors are quite large (generally about two inches in diameter). The
multiple forms of a cancerous glial cell also make it difficult to
identify and locate all of the cells tendrils. Removal or destruction
of the main tumor mass while leaving these tendrils intact is
ineffective therapy: like the mythical Hydra, the tendrils will sprout
new tumors.
Glioblastoma multiforme is a cancer of the glial cells,
the cells that provide physical and chemical support for neurons.
Approximately 90-percent of all the cells in the central nervous system
are glial cells which, unlike neurons, undergo a cycle of birth,
differentiation, and mitosis (cell-division). That they undergo this
cycle, makes glial cells vulnerable to becoming cancerous. When they
do, as the name "multiforme" suggests, they can take on a wide variety
of different shapes, which often makes detection difficult until the
tumors are quite large (generally about two inches in diameter). The
multiple forms of a cancerous glial cell also make it difficult to
identify and locate all of the cells tendrils. Removal or destruction
of the main tumor mass while leaving these tendrils intact is
ineffective therapy: like the mythical Hydra, the tendrils will sprout
new tumors.
The basic technique behind BNCT as a means of destroying a glioblastoma multiforme tumor and all of its extending tendrils was actually proposed more than 60 years ago, shortly after the discovery of the neutron in 1932. The neutron is one of the two types of subatomic particles called "baryons" found in the nucleus of an atomthe other is the proton. A neutron has about the same mass as a proton, but unlike the positively-charged proton, it has no electrical charge. Because they are electrically neutral, neutrons readily penetrate the charged field of an atomic nucleus. This influx of energy can trigger a fission reaction, causing the nucleus to break apart and releasing radiation (imagine a cue ball striking a rack of billiard balls).
Upon the neutrons discovery, physicists began bombarding atomic nuclei with neutrons to create a variety of fission reactions. From these demonstrations, Gordon Locher, a biophysicist with the Franklin Institute at the University of Pennsylvania, got the idea of fighting cancer with the radiation released when an atom of the element boron absorbs a neutron. He proposed introducing boron-10 into a tumor then exposing the tumor to neutrons. Boron-10 is a non-radioactive, non-toxic isotope that had already been shown to have a strong proclivity for the "capture" or absorption of neutrons (it was soon put to use as a radiation shield in the early geiger counters). When boron-10 nuclei capture neutrons, they become, for a brief instant, nuclei of boron-11 in an excited state. The excited boron-11 nuclei immediately fission, producing helium nuclei (alpha-radiation) and lithium ions. Both of these charged particles are high in energy but short in range, which means they destroy the malignant cells in which boro
By 1941, studies of BNCT on mice had shown sufficient promise to move the research forward, but U.S. involvement in the war delayed the start of clinical trials on humans until 1951. A series of collaborative tests were undertaken by researchers at Brookhaven National Laboratory (BNL) and the Massachusetts Institute of Technology (MIT). By 1962, a total of 69 patients diagnosed to be in the advanced stages of brain cancer had received BNCT treatments. Though none of the patients could be saved, autopsies revealed that the treated tumors had been destroyed. Nonetheless, the trials were judged unsuccessful and were abandoned.
The clinical failures of yesteryear are primarily attributed to insufficient knowledge and immature technology, according to Bill Chu, a physicist in the Life Sciences Division (LSD) who works with the Ion Beam Technology Group in the Accelerator and Fusion Research Division (AFRD) and coordinates BNCT research at Berkeley Lab.
"In the early clinical trials, for example, researchers did not know how much boron-10 was in the tumor and the surrounding healthy tissue as they could not measure it," Chu says. "In the end, there was too much damage to the normal tissue for BNCT to work."
Boron-10 must be carried into the brain as part of a chemical compound that can clear the "blood-brain barrier" that encases and protects the brain from viruses. For those first trials, the boron-10 was carried in borax, a simple inorganic compound that did not selectively accumulate in glioblastoma multiforme tumors.
In addition to the selectivity of the boron-carrying compound, the success of BNCT also depends upon the availability of a neutron beam with a suitable energy spectrum and sufficient intensity. The neutron beams for the early trials were produced via fission processes that take place inside nuclear reactors which were constructed at BNL and MIT specifically for BNCT tests. These reactors produced low-energy or "thermal" neutrons which did not penetrate very deeply into the brain. The results were over-irradiated skin and normal brain tissue, and under-irradiated tumors.
